Then our framework got flipped completely upside down.
In my own mind, several pandemic dates stand out as particular milestones: March 12th, 2020, the day Lincoln Center shut down; also November 9th, 2020, the day Pfizer announced that its Phase 3 trial results showed mRNA vaccine efficacy > 90%. (I cried when I read that, knowing how incredibly game-changing that news could be.) Then, the evening of July 29th, 2021, became another one of those momentous pandemic dates.
Why July 29th? Because that was the night the Washington Post published bombshell revelations about the Delta variant based on a leaked CDC PowerPoint presentation. That was the night we found out the pandemic had changed course again…dramatically.
The framework-flipping thus proceeded very quickly, and that has understandably caused psychological whiplash. We’d all glimpsed the light at the end of the tunnel and we thought we were almost out, but literally overnight the light vanished and the tunnel elongated substantially.
This whiplash is not just my opinion. The world’s Covid-19 experts are saying it verbatim.
“The irony is that things got so good in May and most of June that all of us, including me, were talking about the end game,” said Dr. John Swartzberg, an infectious disease specialist at the University of California, Berkeley. “We started to enjoy life again. [But] within a very few weeks, it all came crashing down.” New York Times reporters Mitch Smith and Julie Bosman continue: “The [Delta] resurgence has left the country exhausted, nervous, and less certain than ever about when normalcy might return.” All three people are describing psychological whiplash, or in deliberate practice terms, the extreme discomfort of having your mental representation utterly scrambled in a very short period of time.
Apoorva Mandavilli, the New York Times’ ace Covid reporter, echoes the very same: “We were really surprised by a bunch of things. One expert I talked to early this spring said to me ‘I think we vaccinated our way out of this pandemic’…. He thought that we were going to continue to see the trend in vaccination that was true at the time…. What we did not expect is the level of vaccine resistance…. We’ve stalled at something like 53 percent of the population vaccinated, almost half of the population unprotected, still vulnerable to the virus. That is just not the same picture we were envisioning [last spring].”
As Americans have struggled to adjust to the whiplash, Atlantic staff writer Amanda Mull published the following piece only 20 short days after the bombshell news: Delta Has Changed the Pandemic Risk Calculus. The subtitle says it all: “If you’re confused about what you can do right now, you should be.”
Renowned epidemiologist Larry Brilliant immediately commented on Mull’s story via Twitter:
You are NOT WRONG. If you’re confused about what you can do right now, you should be. https://t.co/4oQKfnNcYU
— Larry Brilliant MD, MPH (@larrybrilliant) August 18, 2021
Got an email from someone taking issue with me saying breakthrough infections seemed rare — on a podcast that aired three weeks ago.
The pace of information in this pandemic is dizzying.
— Apoorva Mandavilli (@apoorva_nyc) August 19, 2021
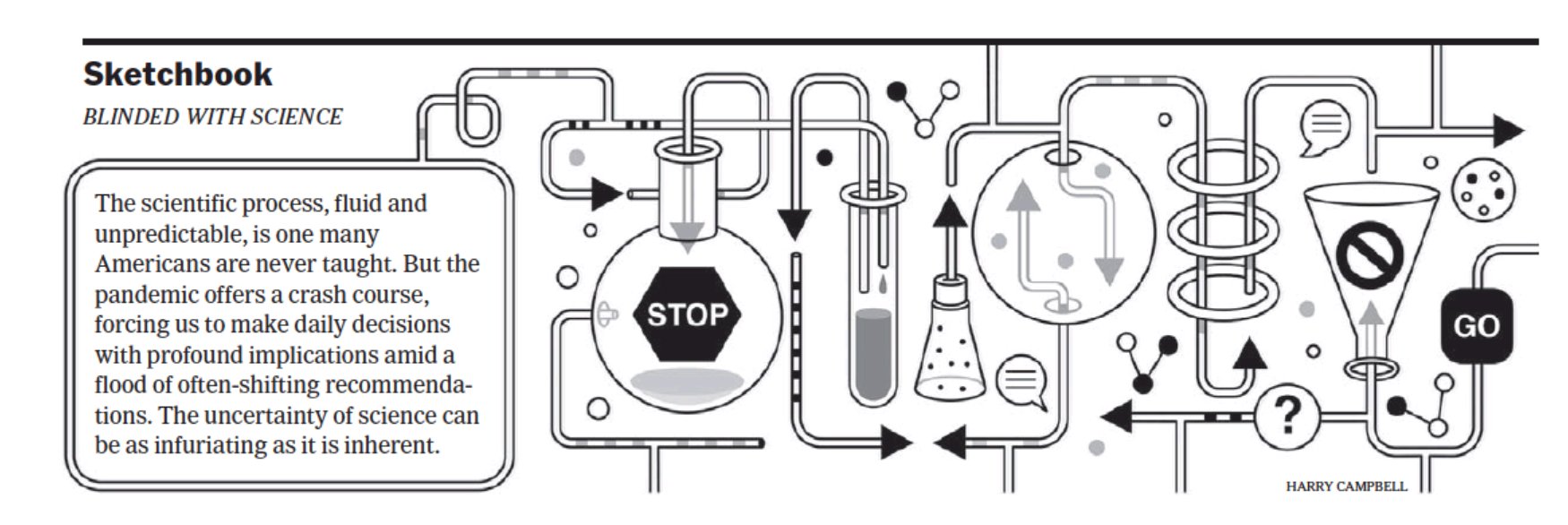
Dizzying indeed. Elaborating three days later, she wrote “The U.S. is getting a crash course in scientific uncertainty. As the pandemic takes an unexpected direction, Americans again must reckon with twists in scientific understanding of the virus.” And another seven days after that, the New York Times Sketchbook illustrated the whiplash as “BLINDED WITH SCIENCE”:
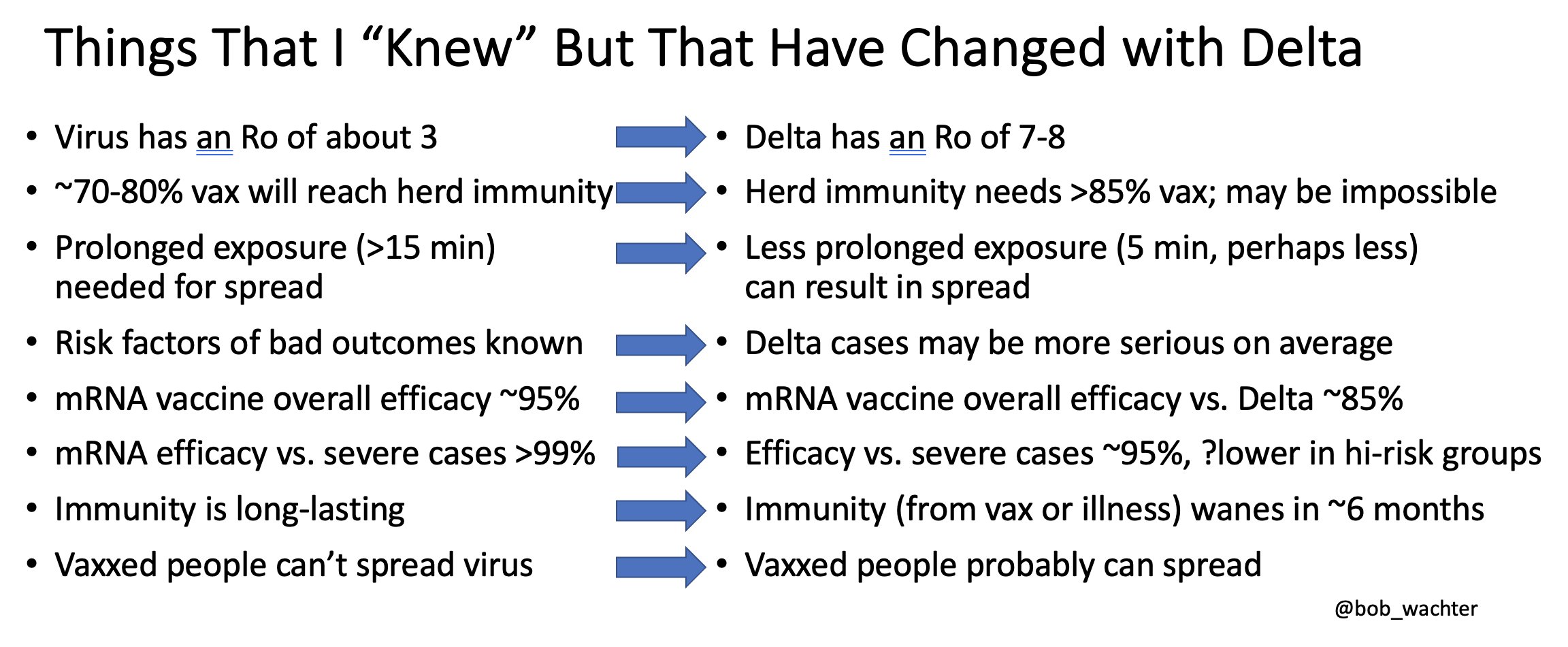
In that interview (and in a subsequent twitter thread), Wachter went on to describe how his own mental model of the pandemic has been humblingly upended by the Delta variant revelations, calling it “cognitive vertigo.” He said that “every new piece of data comes out and often upends what we thought we knew.” Wachter conveniently summarized his thinking in this table:
Most relevant to our current moment, mental representations enable us to respond quickly under pressure. They facilitate what researchers call “adaptive thinking.” Ericsson wrote that mental representations are “preexisting patterns of information — facts, images, rules, relationships, and so on — that are held in long-term memory and that can be used to respond quickly and effectively in certain types of situations. The thing all mental representations have in common is that they make it possible to process large amounts of information quickly, despite the limitations of short-term memory. Indeed, one could define a mental representation as a conceptual structure designed to sidestep the usual restrictions that short-term memory places on mental processing.”
This adaptiveness, quick-thinking, and quick-reacting is absolutely essential. These functions of mental representations enable doctors, athletes, and musicians to “respond without thinking,” “act on instinct,” or “play out of their minds.” Ericsson wrote that the ability “to recognize unexpected situations, quickly consider various possible responses, and decide on the best one…is important…in many areas.”
That ability is important, and it’s exhausting. It requires immense practice. Ericsson continues: “Over time, [experienced surgeons] have developed effective mental representations that they use in planning the surgery, in performing it, and in monitoring its progress so that they can detect when something is wrong and adapt accordingly.” But most surgeons have spent 7–14 years in medical school and residency; the rest of us have had less than 18 months to initially wire and then struggle to rewire our pandemic risk assessment framework.
So it’s worth asking: the pandemic might be confusing again, but why does it feel so bad? I mean, sure, we were all looking forward to Hot Vax Summer, but this letdown feels like something more fundamental. And it is. Because this exhausting rewiring is happening while we’re already fatigued, languishing, or feeling like we’d been swimming (and mostly drowning) for 18 months. It’s emotionally wrenching. In any situation, it’s difficult, painful, stressful, and extremely disorienting when your mental representations are forcibly and rapidly changed. It’s much harder when your gas tank is already empty.
Consider this analogy: On Friday, January 18th, 2013, I arrived at the stage door of the Metropolitan Opera at 10:15 a.m. I signed in for the semifinal round of the principal timpani audition shortly thereafter. I played a long semifinal round (over 17 minutes!). After advancing to finals, I played second out of two finalists, going through nearly every excerpt on the list over the course of almost an hour. By the time I was walking back to the green room to await the jury’s vote, it was almost 6 p.m.
That was a long day: grueling, fraught, and subject to some of the most intense performance pressure imaginable.
But now imagine if the personnel manager had come back into the green room and said “the jury would like to hear candidate number 11 again.” Ummmm…okay?!
Imagine me walking back down those two flights of stairs, re-entering the C-level rehearsal room…and finding completely different timpani. Moreover, they’re now set up “backwards” (i.e., not “American” but “German” configuration). Before I even have a chance to set down my stick case, the jury chair begins barking orders: “Would the candidate please begin the Fidelio excerpt, but this time invert all of the dynamics and articulations, change all quarter notes to 8th notes, and change all 8th notes to 16th notes.”
“Holy hell,” I’m thinking as I race to rewire my entire approach to this excerpt. I try to play, stumbling through, feeling like I’m running the end of a race with my pants around my ankles. Then,
“Would the candidate please play the excerpt from Bartok’s Concerto for Orchestra Movement IV, and without pausing immediately transition to the waltz excerpt from Strauss’s Rosenkavalier.” (These are two challenging “pedaling” excerpts with multiple pitch changes.) “Also, would the candidate please transpose both excerpts down a minor 3rd.”
“What?!” I’m thinking. “This is absolutely insane….” More stumbling, more fumbling. I’m exhausted, and everything is getting worse and worse. Finally,
“Would the candidate please play the iconic Siegfried’s Funeral March from Götterdämmerung, but this time perform it as if Gunther intervenes to stop murderous Hagen, Ragnarök doesn’t happen, Valhalla survives, and Siegfried lives happily ever after with Brünnhilde.”
“Oh — and instead of timpani mallets, would the candidate please use badminton rackets instead.”
“What. The. SHIT?!?!?!” This time, I’d probably scream it out loud as my emotionally shredded self throws down my sticks and collapses onto the floor in an overturned-mental-representation puddle.
That’s what this phase of the pandemic has felt like to me.
We were already fatigued and we thought we knew what to do, but now we have to reconsider everything. Big picture and small scale. Forest and individual trees. Even individual leaves right down to their damn chloroplast cells. Every conceivable avenue of human-to-human contact is once again suspect. Every outing, every time I leave the house — new calculations. Travel plans are out the window. Social hangs are called into question. Every decision has to be reexamined through this new Delta lens.
It just sucks.
Because here’s the problem: you can’t “act on instinct” when the ground has shifted beneath you. You can’t “respond without thinking” when the rug has been pulled out from under you. And you can’t “play out of your mind” when outside forces — new Delta data — have turned your mental model completely upside down.
As the Washington Post originally stated, “the war has changed,” and the Delta variant is “so contagious that it acts almost like a different novel virus.” I’ve even begun thinking about it like this: if the 2020 original virus was like a vicious bobcat, the 2021 Delta variant is more like a full-grown apex predator lion.
To be clear, this is hard enough to make sense of for the world’s finest pandemic experts; it’s absolutely brutal for laypeople to discern the implications of these changes. And it poses particularly acute risks to differing groups at this phase of the pandemic: elderly Americans, who likely got their shots in January–February, and who are now 8+ months down the waning immunity curve; children under 12, who are not yet authorized to be vaccinated; disadvantaged communities lacking access to vaccines, such as disproportionately black and brown Americans living in underserved communities who’ve been consistently overlooked by our medical system for decades; and more proximately in the performing arts, wind players, brass players, and singers, for whom masking while rehearsing or performing is often nonviable.
What are laypeople to do? Well, we erected mental representations of the virus once in 2020, and we can do it again. It will not be easy. But it will be necessary.
(Now, just in case you’ve made it this far and you’re wondering “Why is a drummer writing about the pandemic? He’s not a virologist. Who does he think he is?”…well, fair questions. For a brief recap of my scientific credentials, you can read more here. In previous posts, I’ve referred to my 10 years working as a principal scientist at a nanotech company; relevant to our 2021 circumstances, my prior work involved collaborations with Big Pharma. I always hate “pulling rank,” but it’s worth pointing out that those collaborations necessitated deep dives into medical diagnostics, virology, cell culturing, environmental control systems, HVAC, biocontainment laboratory protocols and designs, semiconductor “class 100” cleanroom facilities, and chemistry wet lab cross-contamination mitigation protocols. So, while I may lack the formal credentials of Drs. Fauci, Wachter, Topol, or Osterholm, I at least have enough experience to know what they’re talking about, and to retranslate for a community invested in deliberate practice.)
So, what are the contours of this new Delta variant terrain? What’s the gist of our new upside down framework? And how has my mental representation of this pandemic rapidly adapted to accommodate our new reality?
1. Transmissibility
This is the headline that drives everything else: Delta’s viral load is >1000x the original virus. This is what makes it so much more contagious, and so much worse in every other way detailed below. (Virologists and epidemiologists quantify transmissibility as the R0 value; Wachter’s table above estimates a new R0 around 7–8, putting it on par with Chickenpox.) And the viral load is extremely high because this variant is exceptionally good at replicating itself very quickly, like the chopped-up brooms in Disney’s Fantasia version of The Sorcerer’s Apprentice. To set up a medieval analogy, it’s as if marauders breach the castle walls at night and the intruders multiply a thousandfold before the guards (i.e., the antibodies of our immune system) even wake up. In fact, the honorable mention for the “Small World in Motion” competition vividly shows this invasive replicating process in its earliest phases:
2. Herd Immunity Depends on Transmissibility
Next, in a blow to our hopes to return to normal, herd immunity becomes much more difficult to achieve with R0 so high and Delta so transmissible. We’d previously assumed the herd immunity threshold was 70–80%; difficult, but doable. Now it may be >>85%…which may turn out to be impossible. That’s why the Atlantic’s Ed Yong wrote “Endemicity was always the likely outcome — I wrote as much in March 2020. But likely is now unavoidable. [Eleanor Murray, an epidemiologist at Boston University, said] ‘Before, it still felt possible that a really concerted effort could get us to a place where Covid-19 almost didn’t exist anymore. But Delta has changed the game.’”
3. More Transmissible Means Less Exposure Time
Throughout 2020, we learned that prolonged indoor exposure greatly increased our chances of infection. A benchmark became “15 minutes or more” for infection. But now that the viral load is 1000x, that exposure time has shortened dramatically. Delta might only need a few minutes of exposure to infect you.
4. Vaccines’ Declining Efficacy Against Infection
You may have already encountered news discussing our vaccines’ decreased “efficacy against infection” (VE). At this point, it’s extremely important to distinguish “infection” from “severe disease.” Infection simply means any marauders inside the castle, whereas severe disease is the castle being overrun or sacked completely. With 1000x the viral load, it’s unsurprising that some Delta marauders will make it over the walls; our immune systems have finite guards, and they’re deployed all over our body. Only a small garrison guards our nasal passages and upper respiratory tract, and so an onslaught invasion there will quickly overwhelm the guards and lead to an initial infection.
How much, then, has our efficacy against infection decreased? Well…it’s complicated. It depends on time (how long ago did you get your shots?), your age and immune system (elderly? immunocompromised?), and which mRNA vaccine you got (Moderna seems to be holding up slightly better, likely because it’s dosed at 100 μg vs. Pfizer’s 30 μg). Studies are all over the map on this. A consensus seems to be emerging around 66%, but some studies have dipped as low as 41%.
How does this translate to rates of breakthrough infections? According to Mandavilli in the New York Times, “breakthrough infections in vaccinated people accounted for at least one in five [>20%] newly diagnosed cases…. [However], these numbers are likely to be underestimates, because most fully immunized people who become infected may not…feel ill enough to seek a test.”
One final point — Pfizer’s initial announcement (VE >90%) actually came with a huge caveat: Phase 3 clinical trial participants were “asked to act as if they were unvaccinated, and keep all other protections in place.” At the time, that meant near-universal masking. So, those initial claims really needed to have been interpreted as “95% when most people are masking.” That obviously stopped being the case when the CDC prematurely relaxed indoor masking for vaccinated people back in May.
5. Thus, the Fully Vaxxed Are Spreaders Again
The second really game-changing headline is that even fully mRNA vaccinated people are once again vectors of transmission. Because even if you don’t develop severe disease, you still have 1000x Delta replicating like crazy in your nasal passages and upper respiratory tract, meaning you’re exhaling infectious virus everywhere all of the time. You might infect your child, or your grandparent, or an unvaccinated member of a disadvantaged community that hasn’t been able to access vaccines.
Related to the VE discussion above, preventing any initial infection has to do with overall levels of antibodies, and this is where we’ve run into trouble: antibody levels decrease after the initial jabs, and therefore breakthrough infections are happening among fully vaccinated people. Worse still, many of these breakthrough infections are asymptomatic — 50% of transmission occurs asymptomatically — meaning the fully vaxxed can be contagious spreaders without even knowing it.
6. Delta Is More Virulent
Imagine two scenarios: an unvaccinated person facing the original virus in 2020, and that same unvaccinated person facing Delta in 2021. How much sicker will they get with Delta? A lot. “Unvaccinated young adults are becoming more severely ill, and more quickly.” How much more? “People who are infected with [Delta] are [at least] twice as likely to be hospitalized.” What about the fully vaccinated? The story here is better: so far, the mRNA vaccines seem to be holding up well against severe disease (which is what they were explicitly designed to do). Against the original virus, protection against severe disease was claimed at >99%; many studies now show ~90% vs. Delta, with some going lower. But the overall picture here still looks okay for the fully vaxxed, for now…
7. There Remain Tens of Millions of Americans Unvaccinated, but Not All by Their Own Choice
Even in September 2021, the unvaccinated are “not all anti-vaxxers.” Underserved communities are exactly that: underserved. “A lot of vaccine information isn’t common knowledge. Not everyone has access to Google. This illustrates preexisting fault lines in our health-care system, where resources — including credible information — don’t get to everyone. The information gap is driving the vaccination gap. And language that blames ‘the unvaccinated’ misses that critical point. Black folks are one of the least vaccinated groups, in part because they have the least access to preventive health-care services.”
Moreover, this group of unvaccinated Americans obviously includes all children under 12, and they number approximately 49 million, leading us to…
8. Delta Is Tougher on Children
Babies and toddlers spread the virus in homes more easily than teens. But children are not just vectors — they’re now getting much sicker. Pediatric wards are overflowing throughout much of the south. New records are being set daily for children hospitalized with Covid. This is tragic.
9. One Negative Covid Test Result Doesn’t Necessarily Mean You’re Safe
A one-off test is not effective at preventing Covid spread. One negative PCR result simply tells you what was very likely true in the past, not today. “This is because the test doesn’t work for Covid contracted in the 4 days leading up to the test. Add that to the delay in getting the test back, and there are now 6 days of potentially risky behavior in which the person could have gotten [and spread] Covid that the test wouldn’t show.” The only way around this is frequent rapid testing, and this has only become more essential with Delta.
10. The Immune System Is Complicated (a.k.a., “The Need for Boosters”)
Ed Yong wrote a piece last summer memorably entitled “Immunology Is Where Intuition Goes to Die.” In it, he describes the complex and often counterintuitive interplay between antibodies, B cells and T cells, and successive shots of vaccine. To extend our medieval siege metaphor, let’s consider the Battle of Helm’s Deep from Tokien’s The Two Towers. “Killer” T cells are massively powerful defenders; think Aragorn, Legolas, and Gimli. By contrast, antibodies are essentially the frontline foot soldiers on the outer walls of the fortress. But the “memory” B cells are truly essential: they have the incredible ability to summon more antibody reinforcements. This would be Gandalf, riding off to find Eomer and the rest of the Rohirrim.
In describing the need for booster shots, Dr. Fauci recently said “it isn’t a question of a vaccine regimen that ‘failed’ where you need a ‘booster’ — I think that a third shot is gonna be part of the original vaccine regimen, just the same as it is with hepatitis, where you have a prime, a second shot after a month, and a third shot at month six.” He notes that this has likely been the correct approach all along; it’s just that it was an emergency to get as many people vaccinated as quickly as possible, so the original trials were designed for a shorter timetable.
With this revised understanding of how SARS-CoV-2 vaccination should have always been working, the first two shots prime the immune system, but the third shot is the serious call to arms, getting our entire immune system mobilized on a sustained war footing. Initial incursions of small bands of orcs had alerted Rohan’s leadership that something was afoot, but it wasn’t until the “third shot” of Gandalf arriving to warn of Saruman’s impending onslaught that we got King Theoden marshalling his forces to the fortress of Helm’s Deep.
In the same interview, Dr. Fauci shared data out of Israel which demonstrated that (a) efficacy against infection was decreasing after only two shots (due to much lower “foot soldier” antibody levels), but more concerningly (b) efficacy against severe disease was waning too, dropping from 99% down to 77%. This implies that the “veteran warriors” were not sufficiently mobilized to begin with. Of those “memory” B cells, Fauci notes that two shots “never got them stimulated enough.” Aragorn, Legolas, and Gimli never reencountered Gandalf the White, and the quartet never made it to Meduseld to warn King Theoden. That is why we need third shots. Fauci concludes that “the effect of the third shot is really impressive…you reconstitute the protection against infection, and you reconstitute the protection against severe disease. And you do that by about tenfold…. The third shot really works…. Three shots is the right combination.” Helm Hammerhand would agree.
11. Long Covid Is Dangerous, and Not Rare
Finally, even if you’re not concerned about spreading the virus to others, and even if you’re willing to live with your fully vaxxed odds of probably not being hospitalized, you’ll want to consider this: Long Covid can be miserable, and it can affect both the vaxxed and unvaxxed who’ve had asymptomatic, mild, or severe infections. “Two-thirds of people with Long Covid say it limits their ability to undertake their day-to-day activities.” Symptoms can include reduced lung capacity, debilitating fatigue, and brain fog so intense that people have had to quit their work-from-home jobs.
Again, any infection at all (regardless of whether your long-term immune system prevents severe disease) carries some risk of Long Covid. Dr. Akiko Iwasaki writes that “you can get Long Covid from breakthrough infection. We don’t know how frequently Long Covid develops in fully-vaxxed people because CDC is not collecting such data. It is dangerous to get breakthrough infections.” And researchers are increasingly confident that Long Covid is “very common, up to 20% of all infections,” with many now suspecting it’s at least 33% of all infections. Even among the fully vaxxed, one study showed that 18% of breakthrough infections led to Long Covid symptoms after six weeks. And asymptomatic infections among fully vaccinated people have led to Long Covid symptoms six months after the initial infection.
But troublingly, we don’t yet have any way to predict which of these afflictions will arise post-infection. Much more research is required on Long Covid, and former CDC director Dr. Tom Frieden puts it succinctly: “There’s a lot we don’t know about Long Covid and why some people still suffer from health problems months after even mild disease. The most certain way not to get Long Covid is to not get Covid.”
***
So, to quote Bo Burnham, this all is…uh…not good.

No use sugarcoating: this is a very bad change-of-course for the pandemic. It’s understandable to wish it were otherwise, but this is the reality we’ve inherited. As I wrote last July, I’m going to continue hoping for the best, planning for the worst, and melding hope with realism.
And this theme should now be obvious: when so many foundational variables have changed in the span of just a few weeks, that can’t not turn our mental representations upside down! Again, as Dr. Wachter said, “if you’re confused, you’re awake.”
This change-of-course is an undeniable setback. But, as with so many of my own experiences on the audition circuit, I think it’s at least valuable to take stock of what we’re learning while we’re suffering. And let me start with this: we got extremely lucky that a small handful of plucky idealistic scientists stuck to their guns 30 years ago, and eventually delivered the mRNA vaccine platform to us despite Big Pharma’s best efforts to sideline them. In particular, “before messenger RNA was a multibillion-dollar idea, it was a scientific backwater. And for the Hungarian-born scientist behind a key mRNA discovery, it was a career dead-end. Katalin Karikó spent the 1990s collecting rejections.”
Dr. Karikó is an Avengers-level hero. And we need to be very clear on this point: the mRNA vaccines are still extremely good at doing what they were designed to do — keep people out of the hospital. That is the heavy lifting of our “veteran” immune systems, the “career military” B and T cells whose long memory will likely sustain durable immunity against severe Covid-19 for years. That has been and will remain the highest priority of our battle against the continuously-mutating SARS-CoV-2 virus.
In spite of the intense confusion of the last six weeks, when we survey the time span from July 29th to now, we’ve actually learned a tremendous amount about Delta in a very short period of time. (I’ve done my best to aggregate this learning in a publicly viewable google document.) In addition to the extraordinary performance of the mRNA vaccines, an extremely smart and intrepid study proved decisively that masking remains extremely effective — even more than we previously knew.
We’ve also learned about the critical importance of indoor air quality, particularly the need for excellent ventilation and rapid air-exchange. We know that when human beings are indoors, we’re inhaling air that’s already been in other people’s lungs, and this can be accurately measured as the “rebreathe fraction.” We’ve learned that for a virus like SARS-CoV-2 that spreads dominantly via aerosol dispersion, we need that rebreathe fraction to be 0.8% or lower; unfortunately, many schools and institutions routinely measure 10–20x that safe level.
We’ve learned that frequent rapid testing is better than infrequent slow testing, even if the slow (PCR) tests are more sensitive. And rapid accurate testing is best of all (e.g., rapid PCR with 4–6 hour turnaround times). We also know that all Covid testing is backward-looking, where the “rearview mirror” can only show us what was true 4–5 days ago.
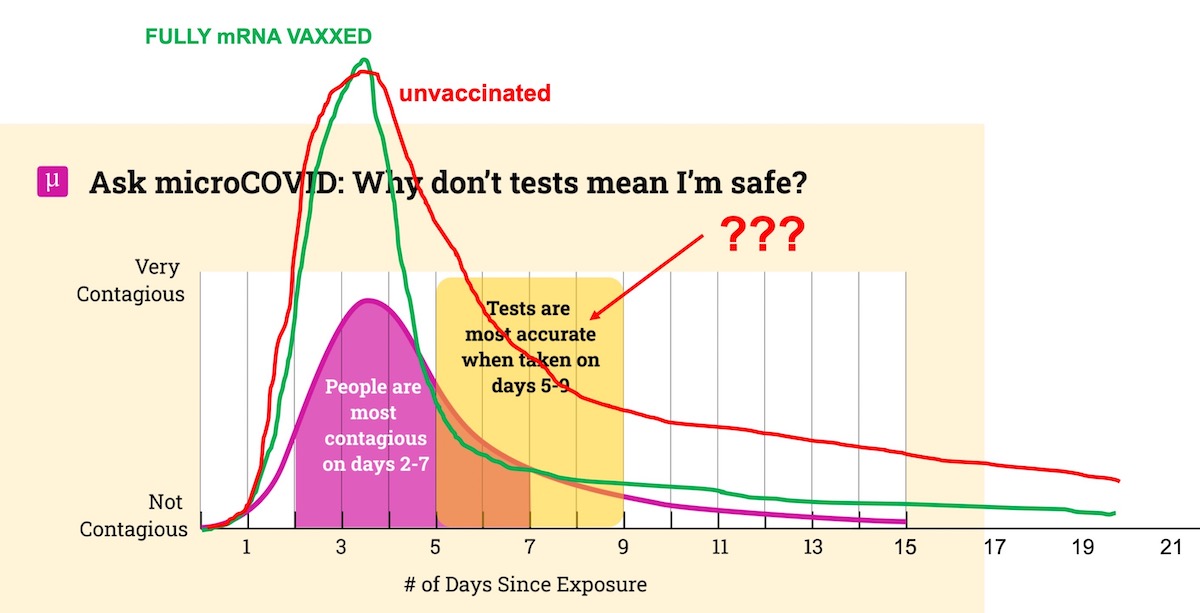
Related, we’re now fairly certain that although Delta viral loads become >1000x higher than the original virus, they also fall off more quickly for fully mRNA vaccinated people “as their immune system responds to quickly clear the virus.” So, while “the potential infectious period lingers much longer in the unvaccinated,” fully vaxxed folks will hopefully be contagious with Delta for a shorter time period.
And finally, we’ve learned the hard way that there’s no silver bullet in this battle; rather, we need to continue conceptualizing risk according to this extremely useful analogy of the “Swiss Cheese” pandemic defense:
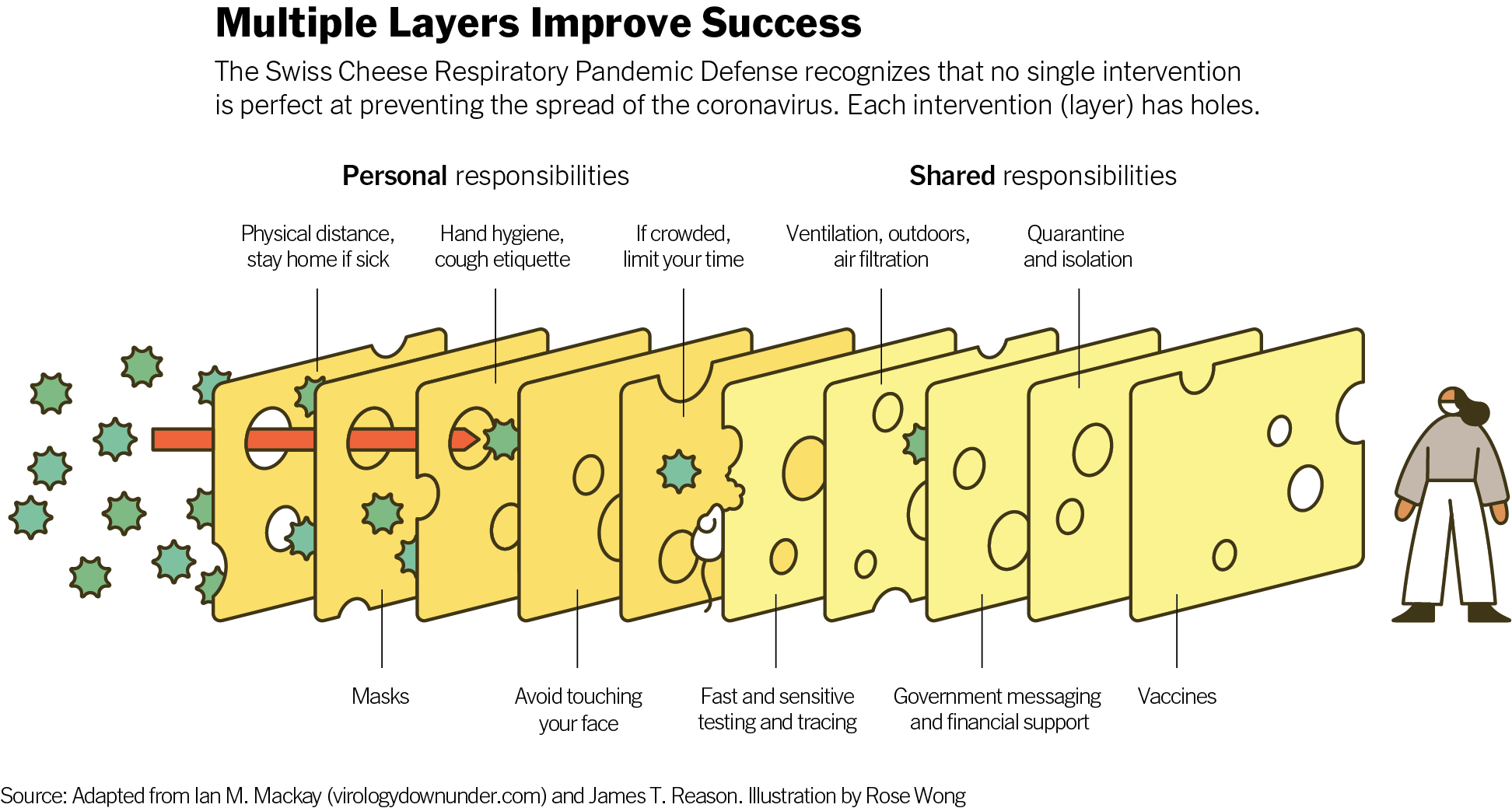
Every slice of cheese matters. Every mitigation layer helps. And while some of these slices are beyond our control (e.g., institutional HVAC controls), others are very much within our control (e.g., masking, frequent testing, and isolation).
This can and should give us hope. There is a way forward, even if it’s not the “return to normal” we were expecting. In honor of the Rolling Stones’ recently departed drummer, the legendary Charlie Watts, I’ll simply offer that “You Can’t Always Get What You Want.”
And here’s the thing: there are tangible rays of hope we can be watching for. Scientists are hard at work developing the next round of vaccines, prophylactics, and therapeutics. Beyond booster shots, there’s promising work being done to develop nasal spray vaccines with variant-specific ingredients. (Per my Helm’s Deep analogy above, this would be like reinforcing the outer walls so that even gunpowder-wielding orcs couldn’t blast them apart.) Coupled with oral antivirals — where Dr. Fauci thinks “we could get at least one of the candidates that are being tested right now…by the end of the year” — and effective therapies to treat Long Covid, these advances could be game-changing. They could return us to the place where the risks to fully mRNA vaccinated people might be much lower, and where we would not be potentially contagious spreaders, thereby enabling a new normal closer to our earlier hopes.So, as Gandalf says to Aragorn and the beleaguered, fatigued, and exhausted remnants of the fellowship before the Battle of Helm’s Deep, “The defenses have to hold…. Look to my coming at first light on the fifth day. At dawn, look to the East.”
.
And just like in The Two Towers, that victory could turn the tide. It will not be the end of the war — this virus and its successor variants will be with us for years — but it could transition us to the next phase, where a mostly vaccinated globe could finally put the end of the war in sight.
![]()